
Allergy Medication Selector
Key Takeaways
- Ketotifen is a mast‑cell stabilizer that works slower but lasts longer than many antihistamines.
- Second‑generation antihistamines (cetirizine, loratadine, fexofenadine) act fast with minimal drowsiness.
- Leukotriene blocker montelukast is useful for exercise‑induced asthma and allergic rhinitis.
- Cromolyn sodium and ketotifen are the only over‑the‑counter mast‑cell stabilizers.
- Choosing the right drug depends on age, symptom speed, sedation tolerance and cost.
When treating allergic conditions, Ketotifen is a mast‑cell stabilizer and antihistamine that helps reduce itching, sneezing and wheeze. It’s been on the market since the 1970s and is available in oral tablets and eye‑drop form.
People often wonder whether ketotifen is the right pick or if a newer antihistamine would do a better job. Here’s your quick Ketotifen comparison with the most common alternatives, arranged so you can see at a glance which drug fits your lifestyle.
How Ketotifen Works
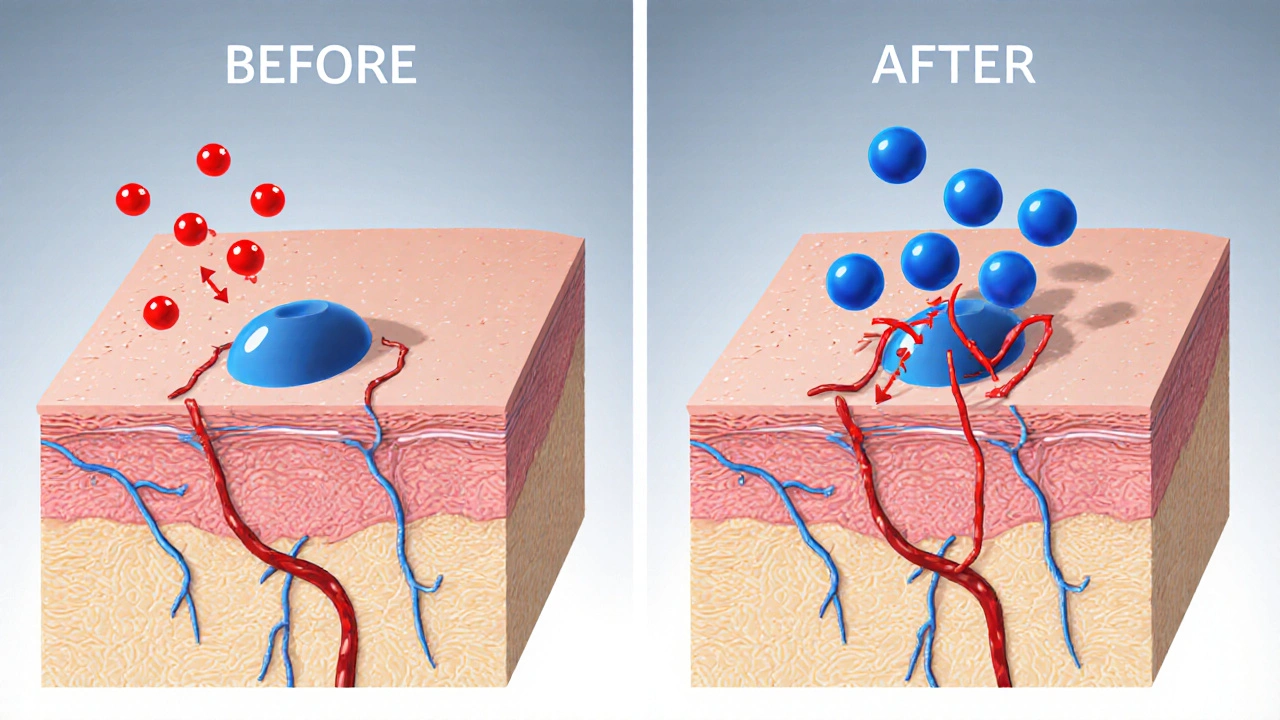
Ketotifen blocks histamine release from mast cells and also binds to H1 receptors, giving it a dual‑action profile. Because it stabilizes mast cells, it prevents the cascade that leads to itching, nasal congestion and bronchospasm. The downside? It needs a few days of regular dosing before you feel the full effect.
Typical adult dosage is 1mg twice daily, taken with food. For children aged 2-12years, a 0.5mg dose is common, but the exact amount should follow a doctor’s advice. Common side effects include mild drowsiness, dry mouth and occasional weight gain. Severe reactions are rare but can include rash or liver enzyme changes, so regular check‑ups are wise.
Overview of Popular Alternatives
Below are brief snapshots of the drugs most often considered alongside ketotifen.
Cetirizine is a second‑generation antihistamine that starts working in 1hour and lasts about 24hours. It’s known for low sedation, though a small percentage of users still feel a bit sleepy.
Loratadine also belongs to the second‑generation class. It has a very clean side‑effect profile, making it popular for daytime use.
Fexofenadine is marketed as a non‑sedating antihistamine that works fastest-often within 15minutes. It’s a good choice for active people who can’t afford any drowsiness.
Montelukast is a leukotriene receptor antagonist. It doesn’t block histamine directly but helps with asthma, allergic rhinitis and exercise‑induced symptoms.
Cromolyn sodium is another mast‑cell stabilizer, available as an inhaler or nasal spray. It needs to be taken before exposure to allergens, similar to ketotifen’s preventive style.
Desloratadine is the active metabolite of loratadine, offering slightly faster onset while keeping the low‑sedation edge.
Levocetirizine is the purified enantiomer of cetirizine, delivering comparable efficacy with marginally lower drowsiness rates.
Side‑by‑Side Comparison Table
| Drug | Class | Primary Use | Onset | Duration | Typical Age | Common Side Effects | Pros | Cons |
|---|---|---|---|---|---|---|---|---|
| Ketotifen | Mast‑cell stabilizer/antihistamine | Allergic rhinitis, conjunctivitis, mild asthma | 2-3days | 12-24h | 2years&up | Drowsiness, dry mouth, weight gain | Prevents flare‑ups, works for both eyes and nose | Slow onset, possible sedation |
| Cetirizine | Second‑gen antihistamine | Seasonal & perennial allergy | ~1h | 24h | 6months&up | Minor drowsiness, headache | Fast relief, once‑daily | May cause slight sleepiness |
| Loratadine | Second‑gen antihistamine | Allergic rhinitis, urticaria | ~1h | 24h | 2years&up | Rare headache, dry mouth | Very low sedation | Can be less potent for severe itch |
| Fexofenadine | Second‑gen antihistamine | Hay fever, hives | 15min | 12-24h | 12months&up | Headache, nausea | Almost no drowsiness | Must be taken with water, not with fruit juice |
| Montelukast | Leukotriene receptor antagonist | Asthma, allergic rhinitis | ~2h | 24h | 6months&up | Headache, abdominal pain | Helps with exercise‑induced asthma | Not a primary antihistamine, may need combo therapy |
| Cromolyn sodium | Mast‑cell stabilizer | Asthma, allergic rhinitis (preventive) | Pre‑exposure | 6-8h | 5years&up | Throat irritation, cough | Works before allergen contact | Needs strict timing, multiple doses |
| Desloratadine | Second‑gen antihistamine | Allergic rhinitis, urticaria | ~1h | 24h | 2years&up | Headache, dry mouth | Fast, low sedation | Higher cost than loratadine |
| Levocetirizine | Second‑gen antihistamine | Seasonal allergies, chronic urticaria | ~30min | 24h | 6months&up | Minimal drowsiness, headache | Strong relief, once‑daily | Prescription‑only in some regions |
What to Consider When Choosing
- Speed of relief: If you need symptoms under control within an hour, second‑generation antihistamines (cetirizine, loratadine, fexofenadine) win.
- Tolerance for drowsiness: Ketotifen, cetirizine and levocetirizine can cause mild sleepiness; fexofenadine and loratadine are virtually non‑sedating.
- Age restrictions: Some drugs (like fexofenadine) aren’t approved below 12months, while ketotifen can be used from 2years.
- Preventive vs. reactive: Mast‑cell stabilizers (ketotifen, cromolyn) work best when taken regularly before exposure. Antihistamines act after symptoms appear.
- Cost and availability: Over‑the‑counter options (ketotifen eye drops, cetirizine tablets) are cheaper than prescription‑only drugs like montelukast in the UK.
Best‑Fit Scenarios
For chronic mild allergic rhinitis that flares with seasonal pollen: Start with a non‑sedating antihistamine like loratadine; keep a rescue dose of cetirizine for breakthrough symptoms.
For children who need a nighttime option without strong sedation: Low‑dose ketotifen taken in the evening can smooth out nighttime itching while keeping daytime alertness.
For exercise‑induced asthma or multi‑trigger allergic rhinitis: Montelukast offers coverage for both leukotriene‑mediated pathways and can be paired with an antihistamine.
For people who need rapid, on‑the‑spot relief (e.g., outdoor events): Keep fexofenadine in a pocket; it works within minutes and won’t make you drowsy.
When you prefer an over‑the‑counter preventive tablet: Ketotifen’s dual action makes it a solid choice, especially if you also suffer from mild allergic conjunctivitis.
Practical Tips & Common Pitfalls
- Take ketotifen with food to reduce stomach upset and improve absorption.
- Never combine two antihistamines unless a doctor advises; the risk of sedation rises sharply.
- If you’re on a medication that slows heart rate (beta‑blockers, certain antidepressants), check with a pharmacist before starting ketotifen or montelukast.
- For nasal spray forms of cromolyn, aim the nozzle slightly away from the septum to avoid nosebleeds.
- Store eye‑drop formulations of ketotifen in a cool, dry place and discard after 30days once opened.
Frequently Asked Questions
Can I use ketotifen and an antihistamine together?
Yes, many doctors pair ketotifen with a second‑generation antihistamine to get both preventive stability and fast relief. Start with low doses and monitor for extra drowsiness.
Is ketotifen safe for long‑term use?
Long‑term studies show ketotifen is well tolerated for up to several years, provided liver function is checked annually. Common side effects stay mild.
Why does ketotifen cause weight gain?
The drug can stimulate appetite slightly and may cause fluid retention. Monitoring diet and staying active usually keeps the gain under control.
Which drug works best for watery eyes?
Ketotifen eye drops are specifically formulated for watery, itchy eyes and often outperform oral antihistamines for that symptom alone.
Can children under 2 take ketotifen?
The UK label restricts use to children 2years and older. For infants, cromolyn nasal spray or pediatric‑dose antihistamines are preferred.
Now you have a clear picture of where ketotifen sits among its peers. Use the decision criteria above, match them to your personal health profile, and you’ll land on the medication that keeps you comfortable without unnecessary side effects.
Author

Bryan Kopp
October 2, 2025 AT 23:16Ketotifen's slow onset just isn’t worth the hassle when a quick fix works.
Patrick Vande Ven
October 3, 2025 AT 01:29Ketotifen functions as both a mast‑cell stabilizer and an H1 antagonist, which distinguishes it from pure antihistamines. Its pharmacokinetic profile requires several days of consistent dosing before maximal effect, a characteristic shared with cromolyn sodium. In contrast, second‑generation antihistamines such as cetirizine or loratadine achieve therapeutic plasma concentrations within an hour, offering rapid symptom relief. The trade‑off lies in sedation: while cetirizine can induce mild drowsiness in a minority of patients, loratadine and fexofenadine are virtually non‑sedating. Cost considerations also differ; ketotifen and cromolyn are generally available over the counter, whereas montelukast often requires a prescription and may be pricier depending on insurance coverage. Age restrictions are notable: ketotifen is approved for children two years and older, whereas fexofenadine has formulations for infants as young as six months. Ultimately, selecting the optimal agent hinges on whether the patient prioritises speed of onset, sedation avoidance, or preventive stability.
Tim Giles
October 3, 2025 AT 03:43When evaluating ketotifen against the broader spectrum of antiallergic pharmacotherapy, it is essential to appreciate the dual mechanism of action that it embodies. By stabilising mast cells, it attenuates the release of histamine, leukotrienes, and other inflammatory mediators at the source, thereby providing a prophylactic shield that many singular antihistamines lack. Simultaneously, its H1‑receptor antagonism affords a secondary line of defense, albeit with a slower onset relative to agents such as cetirizine or fexofenadine, which achieve peak receptor occupancy within 30 to 60 minutes. The clinical implications of this pharmacodynamic profile become evident in scenarios of chronic, low‑grade exposure to allergens, where a patient might benefit from the cumulative protective effect of a mast‑cell stabiliser. However, for acute flare‑ups-especially those triggered by sudden environmental changes-patients may find the delayed therapeutic window of ketotifen unsatisfactory, prompting clinicians to prescribe a rescue antihistamine in parallel. Moreover, the side‑effect spectrum of ketotifen, which includes mild sedation, dry mouth, and occasional weight gain, must be balanced against the virtually non‑sedating nature of newer second‑generation agents. From a pharmacoeconomic perspective, ketotifen's over‑the‑counter availability often renders it a cost‑effective choice, yet this advantage may be offset by the necessity for longer treatment durations to achieve symptom control, potentially increasing overall medication expenditure. Pediatric considerations further distinguish ketotifen; its approval for children two years and older offers a valuable option for younger patients, whereas many antihistamines carry age‑specific restrictions that limit their use in this demographic. Finally, the drug's compatibility with other therapies-such as montelukast for exercise‑induced bronchospasm-highlights the importance of individualized treatment regimens that integrate multiple mechanisms of action to optimise patient outcomes. In summary, ketotifen occupies a niche that bridges preventive and reactive therapy, making it a versatile, though not universally optimal, component of allergy management.
Peter Jones
October 3, 2025 AT 05:56Ketotifen’s preventive angle is handy for folks who can plan ahead, but if you need instant relief, a second‑generation antihistamine is usually the better bet. The side‑effect profile is pretty mild, though a touch of drowsiness can show up. Overall, it’s a solid addition to the allergy toolbox.
Gerard Parker
October 3, 2025 AT 08:09For anyone considering ketotifen, keep these practical tips in mind: take the tablet with food to improve absorption and reduce stomach upset; never stack it with another antihistamine unless a physician explicitly says it’s safe, as you’ll just amp up the sedation risk; monitor liver enzymes periodically if you’re on long‑term therapy, because rare hepatic effects have been documented; and if you’re also dealing with asthma, pairing ketotifen with a leukotriene blocker like montelukast can provide broader coverage. Cost‑wise, the over‑the‑counter formulation tends to be cheaper than prescription‑only options, but be aware of insurance formularies that might favour branded antihistamines. Lastly, if you’re a parent, remember that ketotifen is approved for kids age two and up, making it a viable nighttime option for younger allergy sufferers.
Thomas Burke
October 3, 2025 AT 10:23Ketotifen works slow but lasts long. Good for nightly dosing if you can wait a few days.
Debbie Frapp
October 3, 2025 AT 12:36I appreciate how the article breaks down the onset times for each drug; it really helps when you’re juggling work and school. The point about ketotifen being useful for both eyes and nose is something I hadn’t considered before. It’s also reassuring to see the safety data for kids – that was a major concern for my family. For those who need quick relief during a hike, fexofenadine remains the go‑to, but having a preventive pill on the shelf is a smart backup. Overall, this comparison gives a clear roadmap for tailoring therapy to individual lifestyles.
Michelle Abbott
October 3, 2025 AT 14:49Honestly, the ketotifen piece feels like a lukewarm PR dump – jargon heavy, no real deep‑dive into pharmacodynamics. The “pros” list is basically a re‑hash of marketing hype.
Heather Jackson
October 3, 2025 AT 17:03OMG this post is sooo helpful!! I looove how it breaks down the meds – finally something that makes sense!!!
Akshay Pure
October 3, 2025 AT 19:16The comparative analysis presented herein suffers from an overt reliance on superficial efficacy metrics, neglecting a rigorous exploration of receptor affinity differentials and downstream signaling pathways. Moreover, the author’s omission of pharmacogenomic considerations renders the discussion incomplete for a discerning clinician.
Steven Macy
October 3, 2025 AT 21:29Reading through the data, one is reminded that allergy management is as much an art as it is a science. The balance between immediate comfort and long‑term stability mirrors many life decisions: quick fixes versus sustained habits. Ketotifen’s preventive nature invites patience, while antihistamines reward immediacy. Choosing wisely often means aligning the medication’s temporal profile with one’s own rhythm of exposure.
Matt Stone
October 3, 2025 AT 23:43Ketotifen is okay if you can wait.
Joy Luca
October 4, 2025 AT 01:56From a mechanistic standpoint, ketotifen’s dual‑action provides a synergistic blockade that can reduce both histamine surge and mast‑cell degranulation – a pharmacodynamic advantage worth noting when constructing combination regimens.
Jessica Martins
October 4, 2025 AT 04:09The table formatting makes comparison effortless, especially the clear delineation of onset versus duration. It’s a handy reference for anyone juggling multiple prescriptions.
Doug Farley
October 4, 2025 AT 06:23Sure, ketotifen is a “miracle” if you love waiting days for it to work.
Jeremy Olson
October 4, 2025 AT 08:36The balanced overview respects both efficacy and safety, offering a pragmatic guide for clinicians and patients alike.
Ada Lusardi
October 4, 2025 AT 10:49Great guide! 👍👍 Really helped me pick the right med for my allergy season 🌸
Pam Mickelson
October 4, 2025 AT 13:03Loving the friendly tone of this piece – it makes a typically dry topic feel approachable. The tips on taking ketotifen with food are spot‑on, and the reminder about not mixing antihistamines saved me from a potential headache. Thanks for the clear, upbeat rundown!
Joe V
October 4, 2025 AT 15:16While Gerard’s advice on dosing is solid, it’s worth noting that some patients report breakthrough symptoms despite adherence, suggesting a need for adjunct therapy.
Scott Davis
October 4, 2025 AT 17:29True, combination therapy can be the key for refractory cases.