When a doctor gives you a biosimilar drug-like Inflectra instead of Remicade-how does the system know how much to pay? It’s not as simple as handing over a generic pill and calling it a day. Biosimilars are biologic drugs, made from living cells, not chemically synthesized like traditional generics. That means their billing and reimbursement under Medicare Part B follow a completely different set of rules. And if you’re a provider, pharmacist, or even a patient trying to understand why your bill looks strange, knowing how this works can make all the difference.
How Biosimilars Are Coded: Q-Codes and J-Codes
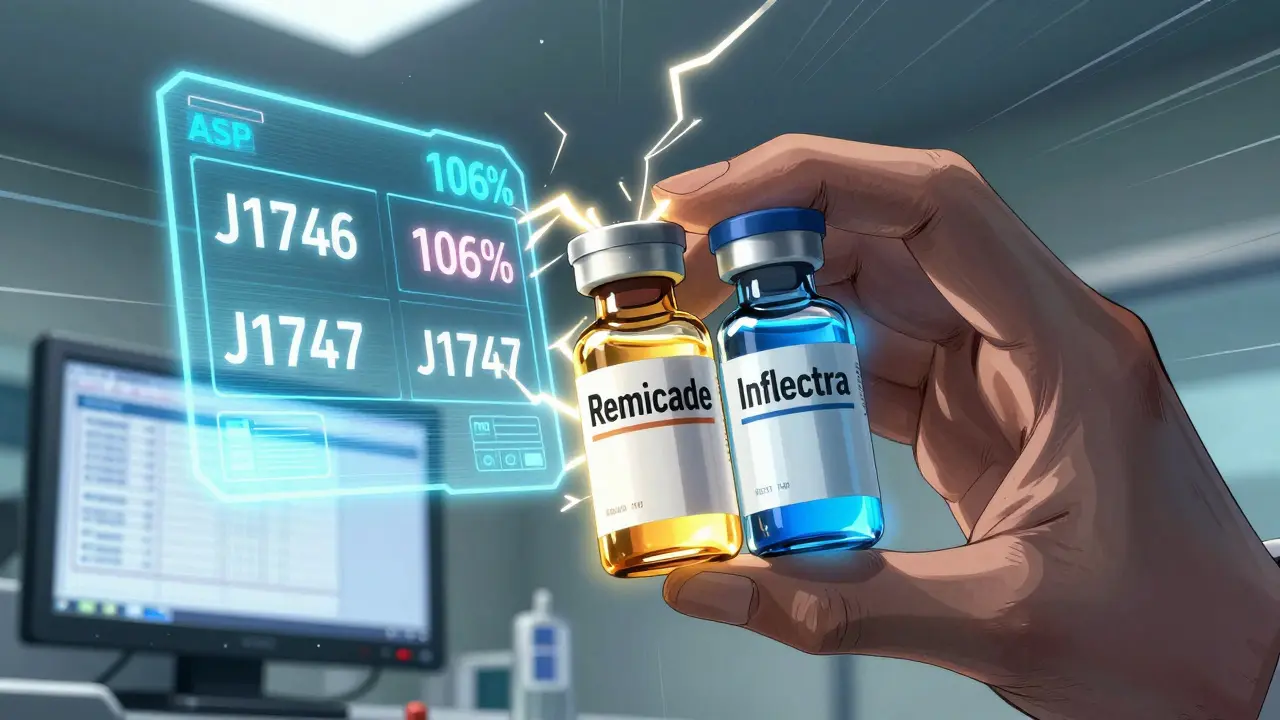
Every biosimilar gets its own unique billing code. Unlike generics, which often share a single code with their brand-name counterpart, each biosimilar has its own HCPCS code. These are either Q-codes (temporary) or J-codes (permanent), assigned after FDA approval. For example, Inflectra (infliximab) has J1746, while Renflexis has J1747. These codes aren’t just labels-they directly determine how much Medicare pays.
This system replaced the old blended model used between 2016 and 2017, when all infliximab biosimilars shared one code (Q5101). Back then, providers got paid based on the average price of all biosimilars in that group. That created a problem: if one company priced its biosimilar low, others could ride on that lower payment without cutting their own prices. The 2018 shift to individual codes fixed that. Now, each biosimilar’s payment is tied to its own Average Selling Price (ASP), not a mix of competitors’ prices.
How Medicare Pays for Biosimilars: The 106% Rule
Medicare Part B pays for all biologics-including biosimilars-at 106% of ASP. That’s 100% of the drug’s actual selling price, plus a 6% add-on. This add-on was meant to cover the cost of handling, storing, and administering these complex drugs in clinics. But here’s the catch: the 6% is calculated based on the reference product’s ASP, not the biosimilar’s.
Let’s say Remicade sells for $2,500 per dose. Its biosimilar, Inflectra, sells for $2,000. Medicare pays the provider 106% of $2,500 for Inflectra-that’s $2,650. Even though the biosimilar cost $500 less, the provider still gets paid as if they gave the brand-name drug. That $30 difference per dose ($265 vs $212) is pure profit for the provider. It’s no surprise that many clinics still default to Remicade, even when biosimilars are cheaper.
This structure was designed to encourage biosimilar entry, but it’s backfiring. Providers earn more per dose from the more expensive drug. A 2020 analysis by Dr. Mark Trusheim at MIT found this incentive directly slows adoption. If the add-on were based on the biosimilar’s own ASP, providers would have a real financial reason to switch.
The JZ Modifier: A New Layer of Complexity
In July 2023, CMS added another layer: the JZ modifier. This is required on all infliximab and biosimilar claims when no drug is discarded. If a vial contains 100 mg and you use 95 mg, you’re not supposed to bill for the leftover 5 mg. The JZ modifier tells Medicare: "I used everything. No waste. Don’t overpay."
But this created a new headache. Gastroenterology clinics now spend 30% more time on billing paperwork just to document discard amounts. One practice reported their staff spent an extra 10 hours a week just verifying vial usage. It’s a well-intentioned rule meant to prevent overbilling, but it’s adding administrative strain without solving the bigger issue: why providers aren’t switching to cheaper drugs in the first place.
Why Biosimilar Adoption Is Still Low in the U.S.
The U.S. biosimilar market hit $12.3 billion in 2022, but that’s only 18% of the total biologics market. Compare that to Europe, where biosimilars make up 75-85% of the market for the same drugs. Why the gap?
- Reimbursement structure: The 6% add-on tied to the reference product’s price disincentivizes switching.
- Payer variation: Medicare Advantage plans and commercial insurers often pay differently than traditional Medicare, creating confusion.
- Provider habits: Many clinicians stick with what they know, especially if they’re paid more to do so.
- Marketing and education: Patients and providers still don’t fully trust biosimilars, even though they’re proven safe and effective.
By 2023, only 35% of infliximab prescriptions in the U.S. were for biosimilars. In Germany? Over 80%. The difference isn’t just about cost-it’s about how the system rewards behavior.
What Providers Are Doing to Get It Right
Successful clinics have built systems to avoid billing errors. One study from the Community Oncology Alliance found that practices using a dual verification system-where pharmacy staff check the administered product against the billing code before submission-cut claim denials from 12-15% down to under 3%.
They also:
- Use manufacturer guides (like Fresenius Kabi’s 2023 coding handbook) to stay current with code changes.
- Train staff for 40-60 hours during major policy shifts.
- Track CMS’s quarterly updates to the Physician Fee Schedule, which are published in January, April, July, and October.
Still, 58% of providers say CMS’s official guidance is "technical but incomplete." There’s no central, easy-to-use dashboard. You have to dig through PDFs, cross-reference codes, and call Medicare contractors when something doesn’t match.
What’s Next? Potential Reforms
There’s growing pressure to fix the system. MedPAC, the Medicare Payment Advisory Commission, has proposed two major changes:
- Consolidated billing: Group all biosimilars and reference products under one code and pay 106% of the weighted average price. This would remove the incentive to use the expensive brand.
- Eliminate the reference product ASP from the add-on: Pay 106% of the biosimilar’s own ASP. That alone could boost adoption by 15-20 percentage points, according to Avalere Health.
CMS is reviewing these ideas. A February 2023 notice asked for public feedback on whether to replace the 6% add-on with a fixed dollar amount. If implemented, this could be the biggest shift since 2018.
Without change, analysts predict U.S. biosimilar adoption will plateau around 40-45% by 2030. With reform, it could hit 65-70%. The tools are here. The science is solid. The question is whether the system is designed to help patients-or just protect profits.
Real-World Impact: What This Means for Patients
For patients, this isn’t just about billing codes. It’s about cost. Even if a biosimilar is 20-30% cheaper, your out-of-pocket cost might not change much. Why? Because Medicare Part B coinsurance is 20% of the payment amount, not the drug’s cost. If you’re given Inflectra but billed at Remicade’s price, you pay 20% of $2,650-not $2,000.
That means patients are still paying more than they should, even when biosimilars are used. And if providers keep choosing the more expensive drug because they earn more, patients never get the full savings.
It’s a system that technically works-but doesn’t always work for the people it’s supposed to serve.
Author

Chris Bird
March 9, 2026 AT 19:50So let me get this straight - Medicare pays more for the cheaper drug? That’s like paying full price for a knockoff sneaker because the original costs more. No wonder no one switches. This isn’t healthcare - it’s a casino where the house always wins.
Randall Walker
March 10, 2026 AT 13:58Wow. Just... wow. So the system literally rewards providers for using the MORE expensive option?? Like, what even is the point of having biosimilars if the incentive structure is designed to keep people on the brand-name stuff? This isn't innovation. This is a joke wrapped in a bureaucracy.
LiV Beau
March 10, 2026 AT 23:43Okay but can we just take a second to appreciate how wild it is that we're using coding systems from the 90s to handle 21st-century biologics?? 😅 Like, we have CRISPR and mRNA vaccines, but billing is still a maze of Q-codes and JZ modifiers?? I’m exhausted just thinking about it. Someone please build a simple app for this. 🙏
Denise Jordan
March 11, 2026 AT 21:18Why are we even talking about this? Just let the market decide. If people want to pay more for Remicade, let ‘em. It’s not like patients are lining up to get ripped off.
Gene Forte
March 13, 2026 AT 07:49Every system is a reflection of its values. If we value profit over patient access, then this system is working exactly as intended. But if we value health equity, then we must admit - this isn’t just broken. It’s immoral.
Kenneth Zieden-Weber
March 13, 2026 AT 18:57So the JZ modifier is basically Medicare’s way of saying "Hey, don’t be lazy - count every last drop of drug in that vial." Meanwhile, the 106% rule says "Hey, just keep billing like you’re giving out gold bars." It’s like a therapist telling you to "communicate better" while your partner keeps stealing your snacks. The contradictions are exhausting.
David L. Thomas
March 15, 2026 AT 10:07The ASP model is a classic example of unintended consequences. You incentivize volume, not value. Providers aren’t greedy - they’re rational actors responding to a broken incentive structure. Fix the payment, not the behavior. It’s economics 101.
Bridgette Pulliam
March 17, 2026 AT 01:30It’s fascinating how such a technically sophisticated drug class - with clinical equivalence proven across multiple studies - is held back by such archaic, opaque, and inconsistent administrative mechanisms. This is not a scientific problem. This is a governance failure.
Mike Winter
March 18, 2026 AT 03:37Interesting. The UK and EU don’t have this mess because they negotiated bulk pricing upfront. Here, we let each drug fight for its own reimbursement slot - like a gladiator arena for pharmaceuticals. It’s inefficient. And frankly, it’s a bit undignified.
Miranda Varn-Harper
March 18, 2026 AT 23:19Let’s be honest - this entire system was designed by consultants who’ve never met a patient. The 6% add-on? A bureaucratic fig leaf. The JZ modifier? A paperwork nightmare. The fact that patients pay 20% of the brand price even when they get the biosimilar? That’s not a loophole. That’s theft.
Donnie DeMarco
March 20, 2026 AT 12:13Bro this is why I hate healthcare. One minute you’re saving money, next minute you’re paying for someone’s lunch because the system’s got more layers than a wedding cake made of bureaucracy. I’m not even mad - I’m just… tired. Like, can we just pay the bill and move on??
Tom Bolt
March 20, 2026 AT 22:50Someone at CMS is laughing right now. "Look at these poor saps trying to code J1746 vs J1747 while patients bleed cash." This isn’t a policy - it’s performance art. And we’re all the extras.
Shourya Tanay
March 21, 2026 AT 10:09As someone from India where biosimilars are the norm, I’m shocked at how convoluted the U.S. system is. Here, biosimilars are cheaper, accessible, and trusted. In the U.S., the problem isn’t science - it’s incentives, marketing, and a reimbursement model that rewards complexity over clarity.
Adam Kleinberg
March 22, 2026 AT 15:54Of course the system is rigged. Big Pharma owns the codes. The JZ modifier? A distraction. The real game? They want you to think this is about billing accuracy. Nah. It’s about locking you into their pricing forever. They don’t want competition. They want dependency.
Alexander Erb
March 24, 2026 AT 10:34Y’all are overthinking it. Just use a simple dashboard. Link the code to the drug. Auto-calculate the ASP. Add a 6% buffer. Done. 🤖 Seriously, we have AI that can write poetry - but we can’t automate a billing rule? Come on. This isn’t rocket science. It’s Excel.