
When you start taking opioids for chronic pain, you’re told about the risks: drowsiness, nausea, addiction. But one of the most common and frustrating side effects? Constipation. And it doesn’t go away. Unlike nausea, which fades after a few days, opioid-induced constipation sticks around for as long as you’re on the medication. Up to 95% of people on long-term opioids deal with it. And most doctors don’t talk about it until it’s already a problem.
Why Opioids Cause Constipation (And Why Regular Laxatives Often Fail)
Opioids bind to receptors in your gut, not just your brain. These receptors control how your intestines move, how much fluid gets absorbed, and how quickly food passes through. When they’re activated, your bowels slow down. Secretions drop. Water gets sucked out of stool. The result? Hard, dry, painful bowel movements that feel impossible to pass. Here’s the catch: regular constipation treatments often don’t work well for this. Increasing fiber? Sounds logical, right? But in OIC, fiber can make things worse. Opioids already slow gut movement, so fiber ferments in the intestines, causing bloating, gas, and even fecal impaction. Studies show 25-40% of patients get more symptoms when they try high-fiber diets. Even over-the-counter laxatives like senna or Miralax only help about half the time. Why? Because they don’t target the root cause. They just try to force things along. But if the gut’s muscles are frozen by opioids, pushing harder doesn’t help-it just causes cramping.What Actually Works: The Step-by-Step Approach
Doctors now recommend a clear, step-based plan. It starts before you even take your first opioid pill. Step 1: Assess Before You Start Before beginning opioid therapy, your provider should check your baseline bowel habits. Tools like the Bristol Stool Form Scale (which rates stool from type 1-hard lumps-to type 7-watery) help track changes. If you’re already constipated, you need treatment before opioids are even prescribed. Step 2: Start With the Right Laxatives First-line treatment isn’t random. The best evidence points to:- Polyethylene glycol (PEG) - 17-34 grams daily. This is the gold standard. It draws water into the colon without irritating the gut.
- Bisacodyl or senna - Stimulant laxatives. Use these if PEG alone isn’t enough. Don’t use them long-term unless needed.
| Drug (Brand) | Form | Approved For | Onset of Action | Common Side Effects | Monthly Cost (USD) |
|---|---|---|---|---|---|
| Methylnaltrexone (Relistor®) | Injection | Palliative care, advanced illness | 30 minutes to 4 hours | Injection site pain, dizziness | $800-$1,200 |
| Naloxegol (Movantik®) | Oral tablet | Chronic non-cancer pain | 25 minutes to 24 hours | Abdominal pain, diarrhea | $700-$1,000 |
| Naldemedine (Symcorza®) | Oral tablet | Chronic non-cancer pain | Within 24 hours | Abdominal pain, diarrhea | $500-$800 |
| Lubiprostone (Amitiza®) | Oral capsule | Women, then men (off-label) | 24-48 hours | Nausea (30%), diarrhea (15-20%) | $600-$900 |
What Patients Are Really Saying
On patient forums, the frustration is real. Reddit users in r/ChronicPain say they’ve tried everything: Miralax, senna, prune juice, magnesium, even enemas. Most say none of it lasts. One user wrote: “I take 100mg of oxycodone a day. I’ve been on Miralax for two years. I still go maybe once every 5 days. I feel like I’m carrying bricks inside me.” Methylnaltrexone gets praised for speed-some say relief in under an hour. But the injection is a barrier. People hate needles. And at $1,000 a month, insurance often denies it unless you’ve tried everything else. Naldemedine (Symcorza®) has better ratings. Patients report more consistent relief and no shots. But 38% still get abdominal pain. That’s a trade-off: better bowel movements, but stomach discomfort. The big complaint? Trial and error. No one tells you which drug to try first. You end up spending months testing options, paying out of pocket, and feeling like your body is broken.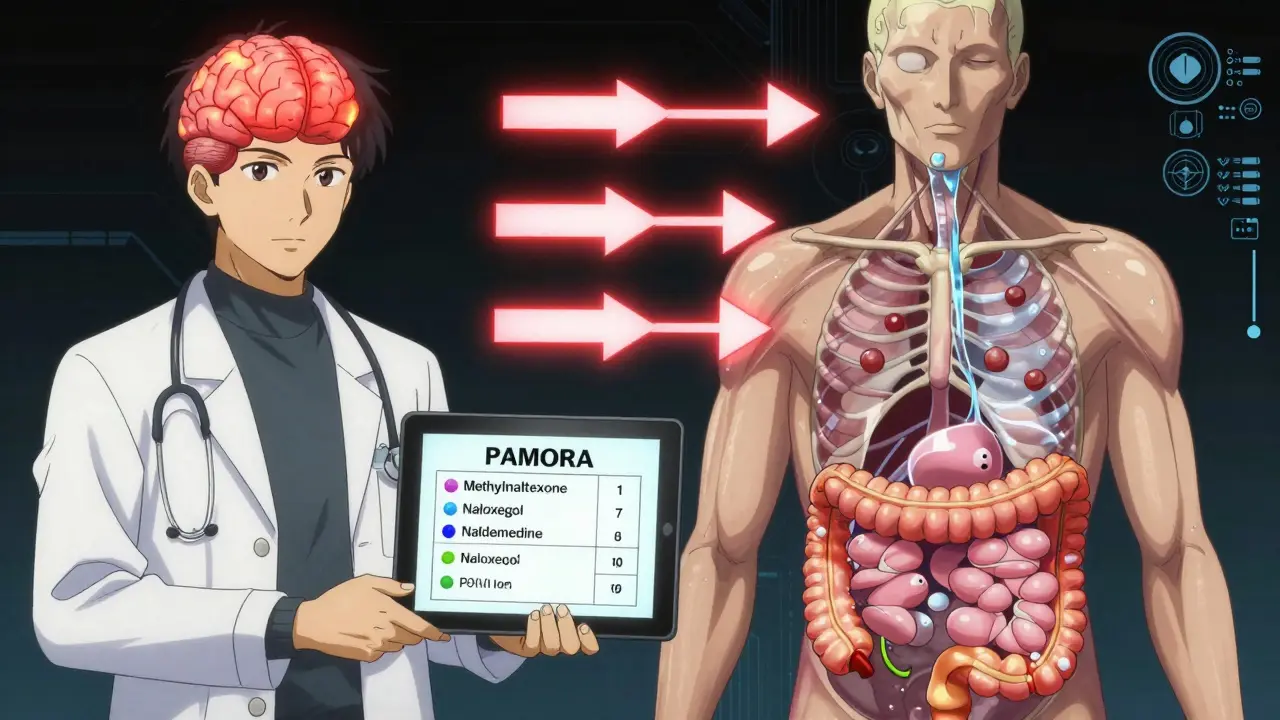
Why So Many People Go Untreated
Even though guidelines exist, most doctors don’t follow them. A 2023 AMA survey found only 22-35% of community practices use standardized OIC assessment tools. Nurses, who see patients daily, say 80% of them would use simpler protocols-but only 19% of doctors agree. Why? Time. Training. Lack of reimbursement. Many providers think, “It’s just constipation. Give them a laxative.” But that’s like treating a broken leg with a bandage. Also, opioids come with FDA-mandated Risk Evaluation and Mitigation Strategies (REMS). Since 2022, these include OIC education. But many prescribers still skip it. The result? Thirty to forty percent of patients reduce or stop their opioids-not because the pain isn’t controlled, but because constipation is unbearable. That’s a huge loss. Pain management fails when bowel function fails.What You Can Do Right Now
If you’re on opioids and struggling with constipation:- Start with polyethylene glycol (Miralax) at 17g daily. Increase to 34g if needed.
- Drink at least 2 liters of water a day. Laxatives need water to work.
- Don’t add fiber unless your doctor says so. It might make things worse.
- Track your bowel movements daily. Use the Bristol Scale. Take a photo if needed.
- If no improvement after 7 days, ask your doctor about PAMORAs.
- Ask if your insurance covers naldemedine or naloxegol. They’re often cheaper than methylnaltrexone.
The Future Is Coming
New treatments are on the horizon. A fixed-dose combo of naloxone and polyethylene glycol is in Phase III trials. If approved in 2024, it could be the first pill that both relieves constipation and reduces opioid tolerance. Also, naldemedine was approved for kids in March 2023. That opens the door for pediatric pain patients-something no one talked about five years ago. The market for OIC drugs is expected to hit $3.4 billion by 2028. More options are coming. But until then, you need to be your own advocate.Frequently Asked Questions
Is opioid-induced constipation the same as regular constipation?
No. Regular constipation is often caused by low fiber, dehydration, or inactivity. Opioid-induced constipation (OIC) is caused by opioids directly slowing gut movement and reducing fluid secretions. Standard treatments like fiber or stimulant laxatives often fail because they don’t address the root mechanism. OIC requires targeted therapies like PAMORAs or osmotic laxatives like polyethylene glycol.
Can I just use Miralax long-term for OIC?
Yes, polyethylene glycol (Miralax) is safe for long-term use in OIC. Unlike stimulant laxatives (e.g., senna), it doesn’t irritate the gut or cause dependency. It’s actually the first-line recommendation. But if you’re still having trouble after 7-10 days at the full dose (34g/day), you likely need a stronger option like a PAMORA. Don’t wait months to ask for help.
Why won’t my insurance cover methylnaltrexone or naldemedine?
Most insurers require step therapy: you must try and fail at least two over-the-counter laxatives and possibly one prescription laxative before approving a PAMORA. Some also require proof that you’ve tried increasing fluid and activity. Your doctor can submit a prior authorization letter citing clinical guidelines and your failed trials. Many patients get approved after one appeal.
Does taking laxatives reduce my opioid’s pain relief?
No, standard laxatives like Miralax or senna don’t interfere with opioid pain relief. They work in the gut, not the brain. PAMORAs like naldemedine and naloxegol are designed to block opioid receptors only in the intestines. They cross the blood-brain barrier too poorly to affect pain control. You can take them safely without losing pain management.
Should I stop my opioid if constipation gets too bad?
Don’t stop on your own. Up to 40% of patients reduce or quit opioids because of unmanaged constipation-even when their pain is under control. That’s dangerous. Instead, talk to your doctor about switching to a PAMORA or adjusting your laxative regimen. There are effective options. You don’t have to choose between pain relief and bowel function.
Next Steps
If you’re on opioids and constipated:- Start tracking your bowel movements today.
- Begin polyethylene glycol at 17g daily.
- Ask your doctor if you qualify for a PAMORA.
- Request a copy of the Bristol Stool Scale to use at home.
- Bring this information to your next appointment. You’re not being difficult-you’re being informed.
Author

Josh josh
January 26, 2026 AT 08:43bro i took oxycodone for a year and just started taking miralax every day and it was like night and day
no more feeling like my intestines are made of concrete
why does no one tell you this upfront
Uche Okoro
January 26, 2026 AT 18:56The pathophysiology of opioid-induced constipation (OIC) is mediated by μ-opioid receptor (MOR) agonism in the enteric nervous system, resulting in reduced peristalsis, increased non-propulsive contractions, and diminished secretory activity-collectively termed 'gut hypomotility.' Standard osmotic laxatives like PEG exert their effect via colonic water retention, bypassing neuromuscular dysfunction. However, the clinical efficacy of PAMORAs such as naloxegol and naldemedine lies in their peripherally restricted antagonism of MORs in the GI tract, preserving central analgesia while restoring colonic transit time. The pharmacokinetic profile of naldemedine, with its high P-glycoprotein efflux and negligible CNS penetration, makes it particularly suitable for chronic non-cancer pain populations. The 2023 JAMA Internal Medicine meta-analysis confirmed a 47% increase in spontaneous bowel movements vs placebo with PAMORA use, with diarrhea as the most common AE (RR 2.1; 95% CI 1.7–2.6).
Joanna Domżalska
January 26, 2026 AT 22:31so you're telling me the real problem isn't opioids
it's that we're not letting people poop
what a revolutionary idea
next you'll tell me water is wet
Henry Jenkins
January 27, 2026 AT 23:15I've been on long-term opioids for 8 years and I've tried everything. PEG works, but only if I drink enough water. I used to think fiber was the answer until I ended up in the ER with a fecal impaction. Now I stick to 34g PEG daily, 3L water, and no fiber. I started naldemedine last year and it's been a game-changer. No injections, no daily struggle. The abdominal pain is mild and worth it. The real issue is that doctors still treat this like a lifestyle problem. It's not. It's a pharmacological side effect that deserves the same attention as nausea or drowsiness. If your doctor doesn't know about PAMORAs, ask for a pain specialist. You're not being difficult-you're being smart.
Mohammed Rizvi
January 28, 2026 AT 00:13man i used to take senna like candy back in the day
thought i was being proactive
turns out i was just turning my gut into a war zone
now i just take miralax and drink water like it's my job
and yeah the docs still act like it's my fault
but at least i don't feel like a brick factory inside anymore
eric fert
January 29, 2026 AT 05:53Let’s be honest-this whole system is a scam. Big Pharma pushes opioids like candy, then sells you $800/month pills to fix the damage they caused. The FDA’s REMS program? A joke. They don’t educate doctors-they just check a box. And now we’re supposed to believe that a $1,000 injection is the solution? Meanwhile, people in other countries get pain relief without this circus. Why are we the only ones treating constipation like a rare disease? It’s not about science. It’s about profit. And the worst part? You’re not supposed to question it. You’re supposed to be grateful for the miracle drug that gives you pain relief and turns your colon into a tomb. And if you complain? They call you ‘non-compliant.’
Ryan W
January 31, 2026 AT 04:35Why are we even talking about this? Just stop taking opioids. It’s 2024. There are better pain meds. Ketamine infusions, nerve blocks, even TENS units. Why are we letting Big Pharma keep people hooked on painkillers that turn their guts to stone? This isn’t medicine-it’s corporate negligence. And don’t give me that ‘but I need it for pain’ crap. If your pain is that bad, go to a real pain clinic. Not some family doctor who thinks Miralax is a cure-all. We’re treating symptoms, not causes. And we’re paying for it-in dollars, in dignity, in bowel movements.
Nicholas Miter
January 31, 2026 AT 11:35Just a heads up for anyone reading this-start PEG on day one. Don’t wait. I didn’t and regret it. I ended up with hemorrhoids from straining for weeks. Also, if your doctor says ‘just drink more water,’ ask them if they’ve ever had OIC. Most haven’t. I had to bring this exact article to my appointment. They were surprised. But they prescribed naldemedine after I showed them the guidelines. It’s not magic, but it’s the best shot you’ve got. And yes, it’s expensive-but call your pharmacy. Sometimes they have coupons. Or ask for samples. Don’t be shy. Your gut deserves better.
Suresh Kumar Govindan
February 2, 2026 AT 08:35This is a controlled experiment in pharmaceutical dependency. Opioids are not for chronic pain. They are for acute trauma. The FDA approved them for long-term use based on flawed studies funded by manufacturers. The constipation? A feature, not a bug. It keeps you compliant. You need the pills to manage the pain. And you need the $800/month pills to fix what the first pills broke. It’s a closed loop. A profit engine. And you’re the product.
TONY ADAMS
February 2, 2026 AT 10:41bro i took 20mg of oxycodone for 6 months and started going once a week
my wife made me go to the doc
they gave me miralax and i cried
not from pain
from relief
why did no one tell me this before
bella nash
February 3, 2026 AT 22:56It is imperative to acknowledge the epistemological limitations inherent in the current medical paradigm, wherein gastrointestinal dysfunction is pathologized as a mere side effect, rather than a systemic consequence of neuropharmacological intervention. The prevailing clinical model, predicated upon symptom suppression via osmotic or stimulant agents, fails to address the ontological disruption of enteric homeostasis induced by exogenous opioid ligands. Consequently, the imposition of PAMORAs, while pharmacologically elegant, remains a palliative intervention within a flawed therapeutic architecture. True resolution necessitates a paradigmatic shift: the de-escalation of opioid reliance, and the reclamation of non-pharmacological modalities of pain modulation, grounded in neuroplasticity and somatic integration. Until such a shift occurs, the patient remains a vessel for pharmaceutical commodification.
Rakesh Kakkad
February 5, 2026 AT 05:51As a physician with 18 years of experience in pain management, I can confirm that the data presented here is accurate and clinically validated. However, I must emphasize that patient education is the most critical missing component. I have seen patients who have been on opioids for 10+ years and never received a single word about constipation until they presented with ileus. I now provide every patient with a printed handout on OIC, including the Bristol Scale and a checklist of first-line agents. Insurance barriers remain the greatest obstacle. I have written over 200 prior authorizations for naldemedine. 87% were initially denied. 92% were approved after appeal. If you are struggling, do not give up. You are not alone. And you are not crazy. This is real. And it is treatable.